Blog
P-PACK, ENLARGED YET CONTRACTED TAPERING DOSE OF PREDNISONECONCLUDES TREATMENT TARGETS FOR PRIMARY SAFETY AND EFFICACYENDPOINTS.
- Efficacy was tolerable across all studied populations with rapid decline in symptoms after
- first dose.
- Effectiveness was achieved, at the end of treatment, across all the therapeutic indications
- that were intervened.
- Safety data during and post treatment revealed no toxicity or hospitalization for acute or
- chronic undesirable pharmacodynamic properties.
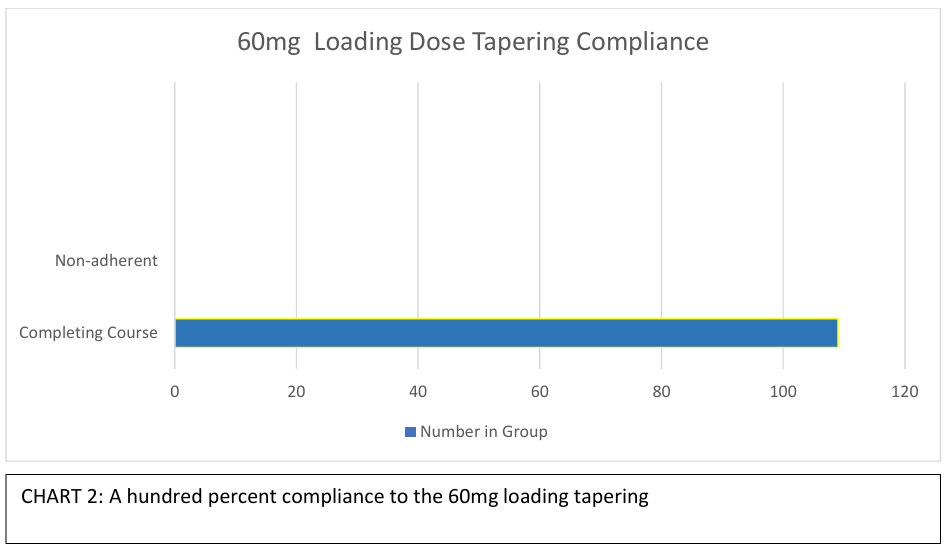
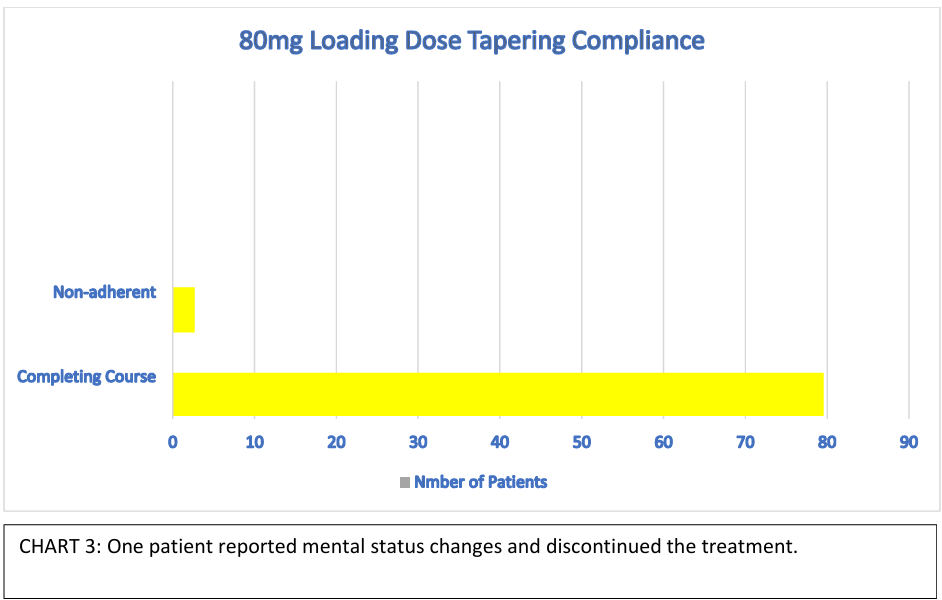
- Acceptance of use measured in compliance or adherence was over nine eight percent.
Abstract
It is common practice in ambulatory medicine and outpatient specialties for doctors and care
practitioners to prescribe a course of glucocorticoids as a crucial armamentarium for symptomatic
disease relief, if there is appropriate use. Yet, there are limited and efficacious options for pre
pack corticosteroid protocols that are effective. Our goal was to test the safety, effectiveness and
efficacy of two tapering prednisone therapies for common disease complaints.
Doses were administered only based on rudimentary data of therapy from specific disease
conditions, and a final balancing for a cardinal pack. To comply with standard of care, patients
received referrals to respective specialists as needed.
Methods: The study cohort consisted of a group receiving 60mg- day- one loading dose of
prednisone with tapering versus the other group receiving 80mg loading dose on day one with a
tapering. Each participant started at a different time when they reported sick and were followed
during the treatments. The end points for the two cohorts on the agents were: dose size response,
complaints of adverse effects and adherence to the course.
Results:
Of a total of 109 patients, 30 received the 60mg initiated tapering dose and 79 received the 80mg loading
dose course. The average age for the participants was forty-eight for which majority was male gender. Of
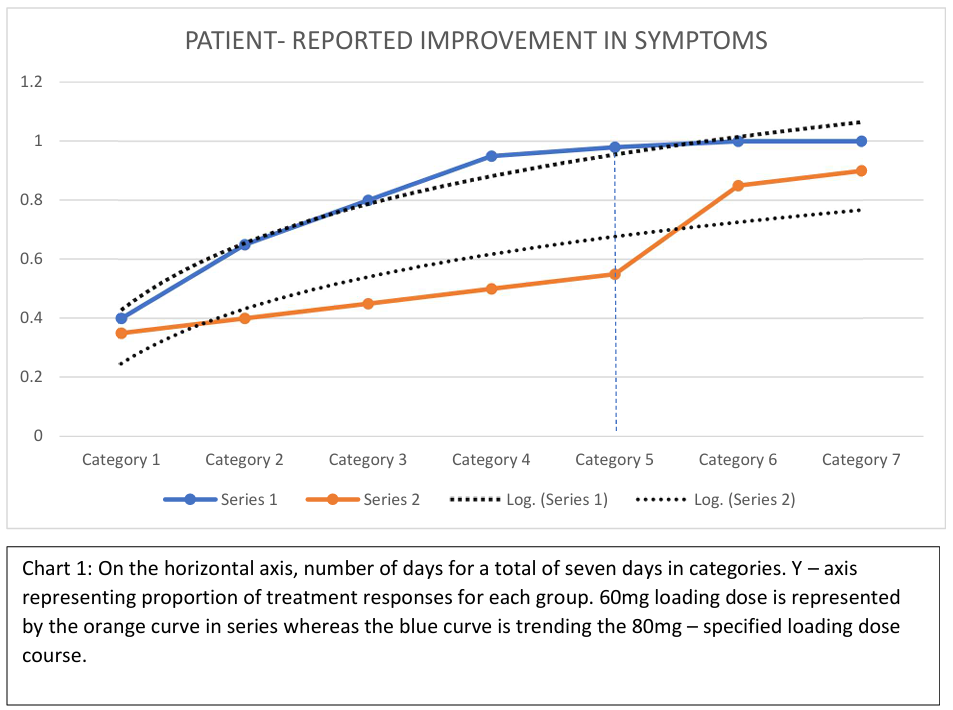
the 30 patients receiving the 60mg loading dose with tapering, the mean of the response is 0.57, with
variance of 0.05 and SD 0.22 CI [0.4101, 0.7327] over the course of the seven days. On the 80mg loading
dose arm, the mean is 0.82 variance of 0.05, SD 0.23 CI [0.6561, 0.9925] . The response percentiles at 25,
50, 75 were 0.43, 0.5, and 0.7 for the 60mg loading dose taper, and 0.73, 0.95, and 0.96 for the 80mg arm.
The two – tailed P value equals 0.0549. At day five, the 80mg loading dose of prednisone was 43% more
effective than the 60mg tapering across all the conditions treated without any adverse events or
hospitalizations. On day three, participants achieved significant recovery for return to work.
Conclusion:
In this study, we have compared tapering doses of prednisone. Across common conditions treated, we
have shown more effectiveness with prescribing four of 20mg on day one to be taken at the same time with morning dosing preferred, three on day number two, and two daily on days three, four and five and
then two daily to complete over seven days for a total count of fifteen.
Introduction
The spending in hospital admissions in the United States, a $ 14101 per admission in 20191and
overall, 3.5 trillion costs between 2012 and 2019,2 stirs a challenge for effective solutions that will
stem this tide. One such solution is the rigorous use of efficient treatments in outpatient services
such as primary care doctor offices and urgent care units.
Common diseases such as ear, nose and throat infections, asthma, chronic obstructive pulmonary
disease, cellulitis, inflammatory cardiac conditions, as a few examples, can rapidly deteriorate into
hospital admissions without swift action; hence ambulatory centers need to match one of the
advantages deployed by Hospitals and that is, use of more pharmacodynamically effective
intravenous therapies.
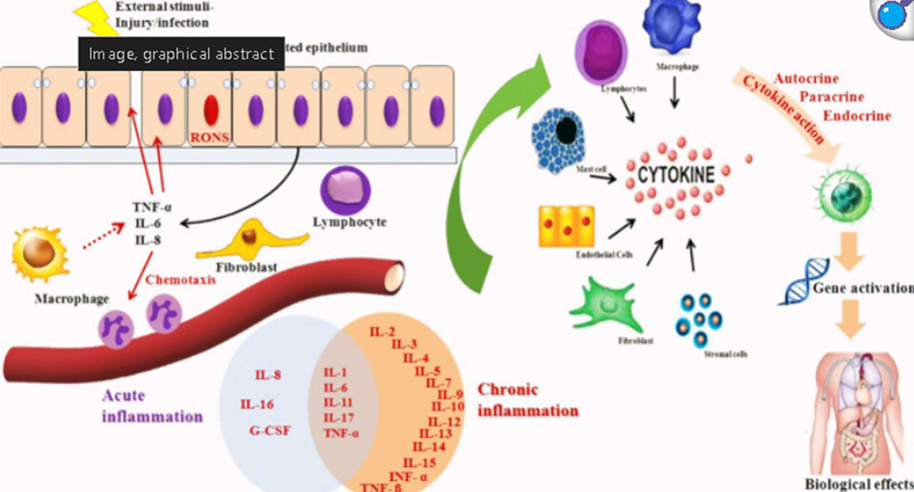
The inflammatory cascade is ultimately a restorative reactive process that commences with
epithelial disruption from tissue injury resulting in a structured formation of dynamic mechanisms
and a smorgasbord of immune-mediating chemoglobulins. The chemical mediators for tissue
protection elicit leukocytes and cytokines production thereby propagating the inflammatory chain
cycle. Post injury, this formation is inevitable: platelet aggregation, macrophages, nitric oxide,
prostaglandins, macrophages, TNF-a, IFN-g, IL-6,IL-8, IL-1, B – cell activation, IL- 10, classes
of cytokine receptors and their cytokines, fibroblast production, transitioning into a chronic phase
with formation of IL2 all the way through to IL-15.3,4. Chronic cytokine involved inflammatory
processes are horrendously perilous by progressively shortening telomere spans, thereby
portending shorter lifespans.
Albeit the function of the immune responses is only natural to curbing tissue – damaging events before a
terminal nadir, their parallel effect leaves patients with fevers, unbearable symptoms of diaphoresis,
severe fatigue, relentless cough, peri-organ effusions with possible hemodynamic collapse,
insomnia, gastrointestinal symptoms and cerebral events. The adrenal gland plays a counter
homeostatic role in producing glucocorticoids to reduce these painful intermediary metabolic
processes. The glucocorticoid production is a six-pathway stream with anti-inflammatory response
through the immune-adrenal axis. Further, each enzyme, receptor and dot on this known
inflammation constellation has been met with drug development. One such medication class that
is shifting the paradigm in patient care is glucocorticoids.
Prednisone is intermediate – acting and advantageous in reducing myopathy associated with other
long-acting glucocorticoids. Prednisone is much less expensive. The dosing conversion of 120mg
of methylprednisolone equals 150mg of Prednisone. Prednisone moderates inflammation by
controlling protein synthesis, suppression migration of polymorphonuclear leukocytes (PMNs),
fibroblast, and restricting lysosomes. The bioavailability is 92 percent with peak plasma time of
two hours for immediate release and 6 hours for delayed release. It is extensively metabolized in
the liver with half – life of 2.6 – 3 hrs. With these known facts, and to be consistent with the law
of reaction mass concentration, a higher dosing pack was tried.
PATIENTS AND METHODS
At the time of patient treatment, informed written consent was obtained. Standards of patient
autonomy and safety were adhered to.
Study Design, Setting and Patient Population
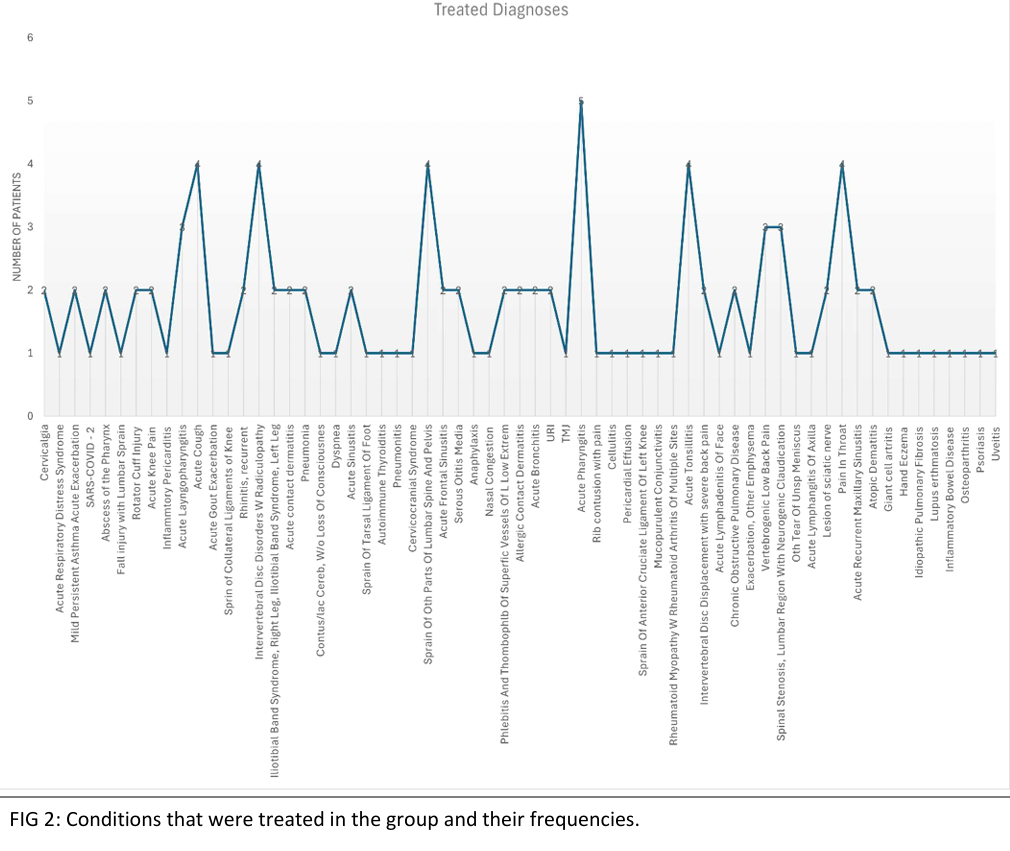
This study was conducted between June 2020 and September 2024. This is an outpatient -based
study of patients presenting with complaints and finally diagnosed to receive treatment for various
conditions involving a systemic corticosteroid. Patients older than 16 years of age were included
in the study. Demographic characteristics recorded were age, gender, and race. Diagnosis for
inclusion was confirmed with patients’ presenting complaints, physical examination and
diagnostic tests that were applicable. Exclusion included osteoporosis, cataract, and pregnant
patients.
In this effectiveness study population, the prospective cohort consisted of a group receiving 60mg
on day one loading dose of prednisone with tapering versus another treatment group receiving
80mg loading dose on day one with the tapering. Each participant started at a different time when
they reported sick and were followed during the treatments. Patients were initially randomized in
a 1:1 ratio to receive either one of the treatment tapering courses. Physician’ s enthusiasm for using
the 60mg loading dose declined during the study.
| DAY | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| 60mg Loading Dose | 60mg | 40mg | 20mg | 20mg | 20mg | 20mg | 20mg |
| 80mg Loading Dose | 80mg | 60mg | 60mg | 40mg | 40mg | 20mg | 20mg |
Data Collection
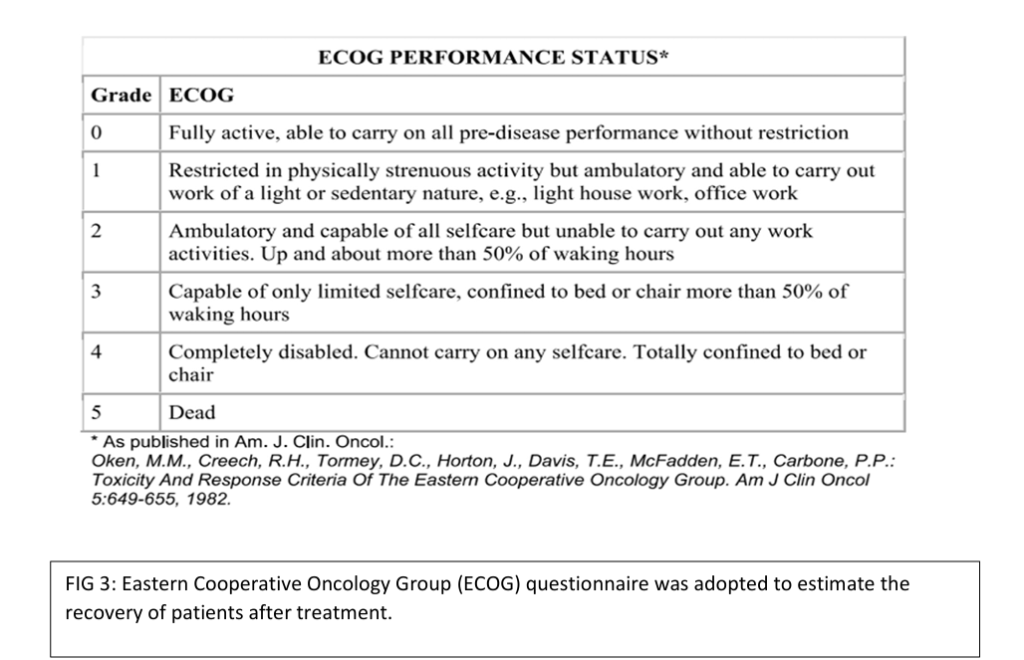
To measure effectiveness, The ECOG performance status questionnaire was used to collect data
post treatment initiation on each arm of the study. Through telephonic questionnaire, patients were
inquired about their symptoms and progress after initiating intake of the medication taper. The
medications had been prescribed by a physician and dispensed by licensed pharmacists in the
community. A few patients also obtained the medications directly through our in-house pharmacy.
Outcomes
Patients were followed for symptomatic improvement, hospitalization and for adverse effects. The end
points for the two cohorts on the agents were: dose size response, complaints of adverse effects and
adherence to the course.
Statistical Analysis and Model Description
Descriptive statistics are provided and tabulated with Microsoft Excel. Our study did not divulge any
personal health information.
RESULTS
The study population comprised of a total of 109 patients with 30 receiving the 60mg initiated tapering
dose and 79 receiving the 80mg loading dose course. The average age for the participants was forty-eight
for which majority was male gender.
Of the 30 patients receiving the 60mg loading dose with tapering, the mean of the response is 0.57, with
variance of 0.05 and SD 0.22 CI [0.4101, 0.7327] over the course of the seven days. On the 80mg loading
dose arm, the mean is 0.82 variance of 0.05, SD 0.23 CI [ 0.6561, 0.9925]
Effectiveness
The 80mg arm showed effectiveness of 0.98 for 78.6 treatments and for the same duration of treatment,
the clinical effectiveness was 0.55 for 16.5 treatments.
Number Needed to Treat NNT,
On average for the 5th day, 2.4 patients would have to receive the 80mg loading taper for one additional
patient to have the study outcome. At day three, most patients reported return-to-work ready.
The response percentiles at 25, 50, 75 were 0.43, 0.5, and 0.7 for the 60mg loading dose taper, and 0.73,
0.95, and 0.96 for the 80mg arm. The two – tailed p value equals 0.0549. The mean of 80mg with tapering
minus that of the 60mg with tapering equals 0.2529. 95% confidence interval of this difference is -0.0062
to 0.5119, using t value of 2.1268 standard of error difference 0.119
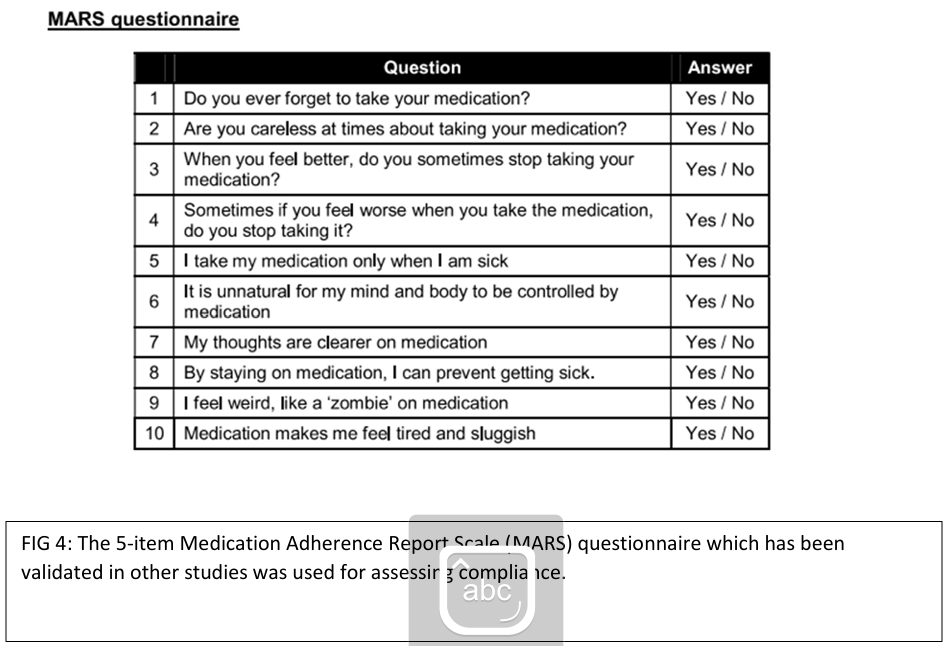
Adherence was addressed by patient self – report of complaints or inquired by the research team. The
team adopted a format of the MARS questionnaire to obtain data on compliance.
Discussion
With increasing patient volumes, practitioners are easily distracted by pre- pack prescriptions, some of
which completely upset the rules of pharmacodynamics and pharmacokinetics that guide proper
prescribing. A situation which may be contributing to the problem of increasing hospitalizations. Perhaps,
keeping a more guiding attention is the right approach.By sampling common intravenous and oral glucocorticoid treatments used at hospitals and outpatient
centers, this study developed two separate tapering doses. By comparison, these two protocoled doses
were deemed moderately high, yet with an appropriate temporal oral intake for seven days. A 60mg
loading dose with taper and an 80 milligram with taper. The difference between the mean of the 60mg
taper and that of the 80mg equals 0.2529, a 95% confidence interval from minus 0.0062 to positive 0.5119.
A two tailed p -value of 0.0549, with some statistical significance; meaning a chance of type 1 error, that
is rejecting a correct H0, is small. The standard error of difference being 0.119. On the 5th day, the larger
loading dose showed superiority in effectiveness than the smaller loading taper, by a difference of 43
percent. The log curve of the higher dose continued over higher area than the lesser dose to the end of
the study.On average, if the 60mg served as a control, then only 2 patients would have to receive the 80mg dose
for one patient to reach the study endpoints. The low number fortifies a more effective therapy with the
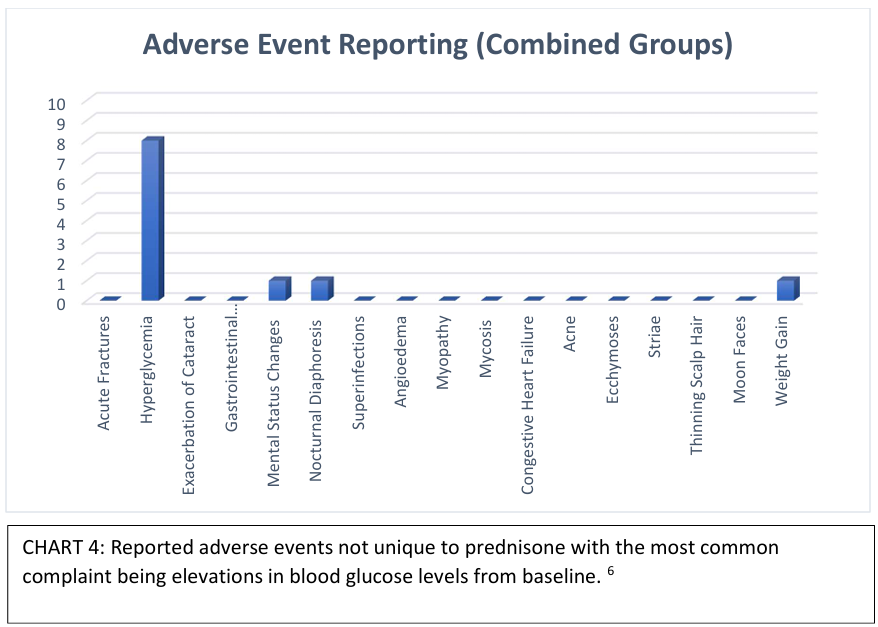
80mg load dose. It is noteworthy that there were no serious adverse events with all reported concerns
already associated with glucocorticoids.Limitations
Although specific disease conditions were treated in this study, understanding the etiology of any case is
necessary in validating the addition of the prescribed 80mg taper in any specific regimen. The study did
not account for confounding factors originating from other medications such as anti-infectives in the
outcomes. Comprehensive assessment of glucocorticoids will require multiple institutional data with
laboratory and imaging analysis for better tracking of the response to treatment.Conclusion
Acute health conditions requiring glucocorticoids are met with doses for which we have shown that there
is opportunity for increasing the dose with better tapering in physician offices; hence the P- PACK 80mg
20mg loading dose shown here in this study with superiority.